
In this article we will discuss about Entamoeba:- 1. Introduction to Entamoeba 2. Etymology of Entamoeba 3. Reproduction 4. Life Cycle 5. Pathogenicity.
Contents:
- Introduction to Entamoeba
- Etymology of Entamoeba
- Reproduction of Entamoeba
- Life Cycle of Entamoeba
- Pathogenicity of Entamoeba
1. Introduction to Entamoeba:
Entamoeba is a parasitic amoeba infecting man. The genus Entamoeba was established by Leidy in 1879.
ADVERTISEMENTS:
Some important species of Entamoeba are described below:
i. E. histolytica (Fig. 1.1E):
Entamoeba histolytica was first reported by Losch (1875) in Russia, but he described it as Amoeba coli. Schaudinn established E. histolytica in 1903 and differentiated the pathogenic and non-pathogenic types. It has a very wide, almost cosmopolitan distribution and occurs especially in the tropical countries where sanitation is in bad state.
It inhabits the mucous and sub-mucous layers of the large intestine of man. It may also occur in the liver, lungs and rarely invades brain, spleen etc. producing ulcers. E. histolytica causes a serious and often fatal disease, known as amoebiasis or amoebic dysentery, the medical importance of which is well established.
ADVERTISEMENTS:
ii. E. hartmanni:
It lives in the colon and invades the intestinal tissues and causes amoebic dysentery but of a less harmful nature than E. histolytica. The diameter of trophozoites are 9 to 14 µm, while that of mature cysts is less than 10 µm.
iii. E. coli:
It is a common endo-commensal found in the colon. It is harmless, generally feeding upon bacteria, particles of undigested food, but rarely on blood cells or other living tissues of the host. The trophozoite measures about 20 to 30 µm and the cyst 15-22 µm in diameter (Fig. 1.7).

iv. E. gingivalis:
It occurs in the mouth of nearly 70% human population and is especially abundant in abscesses of gums, throat and tonsils. They are nonpathogenic, but aggravate the disease by destroying the tissues in gums. They do not form cysts and are directly transmitted from mouth to mouth, during kissing or feeding. Trophozoites are fairly active and measures about 10-20 µm in diameter (Fig. 1.8).

The type which is described in this text is E. histolytica.
2. Etymology of Entamoeba:
Greek: entos, within; amoiba, change or alteration.
The name histolytica (Greek histos, tissue; luein, to dissolve) is given to the parasite because of its power of dissolving the tissues.
Morphology:
There are three stages in the life cycle of E. histolytica, namely trophozoite, pre-cystic and cystic stages.
ADVERTISEMENTS:
i. Trophozoite or Vegetative Stage:
The adult and harmful stage of Entamoeba is called trophozoite (Greek trophe, food; zoon, an animal. The growing or feeding stage). The parasite at this stage nourishes itself at the expense of the host, feeding on the red cells and cytolyses tissues.
The shape of the parasite is not fixed. The size varies from 18 to 40 µm in diameter. The variation in size is either due to the presence of diverse-sized races and strains or due to growth following binary fission. The cytoplasm, in living condition shows two distinct portions — a clear translucent ectoplasm and a granular endoplasm.
The endoplasm often contains ingested red blood corpuscles, whose number may vary from 1 to 10 and are usually smaller in size than the normal. The endoplasm may also contain occasionally leucocytes and tissue debris. Pseudopodia is either long, finger-like or short and rounded in shape (Fig. 1.9).

In freshly passed stool of man the parasite is very active and moves rapidly in a straight line with the help of single pseudopodia at the anterior end. This is known as “directional movement”. When the faces cool down, the movement becomes sluggish and Entamoeba then throws out pseudopodia at various directions and remains stationary.
The inner granular endoplasm contains the nucleus and food particles containing the ingested bacteria, erythrocytes and other substances.” The nucleus is rounded, vesicular and its size is about 4 to 6 µm in diameter. The nucleus is indistinct in living condition but when stained with haematoxylin, it shows a small dot-like central karyosome or endosome (Fig. 1.10).

This central dot is often surrounded by a clear area or ‘halo’, and a relatively fine peripheral layer of chromatin granules. The nucleoplasm sometimes contains traces of linin network in the form of fine fibrils in between karyosome and nuclear membrane. The nuclear membrane is very delicate. Contractile vacuoles are absent as the parasite lives in an isotonic environment and requires no osmoregulation.
ii. Pre-cystic Stage:
When the parasite encounters shortage of food or any unsuitable environment, it assumes a colourless, round or slightly ovoid body with a blunt pseudopodia projecting from the periphery. The ectoplasm is hardly recognisable. The pre-cystic form (Fig. 1.11) is much smaller in size, measuring 10-20 µm in diameter.

Owing to its small size, it is often referred to as E. minuta. At this stage motility becomes slow and finally stops. The nucleus at this stage becomes visible and its structure is much the same as that of the trophozoite stage.
The endoplasm frees itself of food particles such as red cells and tissue debris and in its place glycogen begins to appear. The pre-cystic forms develop into cystic forms, but if they are ejected in the stool no further development can take place.
iii. Cystic Stage:
The cysts of E. histolytica vary in size from 10-20 µm in diameter. When stained in haematoxylin, a matured cyst looks spherical and quadrinucleate. The cytoplasm is clear and often contains black rod-like chromatid bars or bodies with rounded ends (Fig. 1.12).
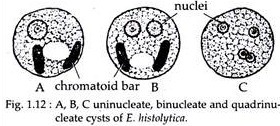
The young cysts are either uninucleate, bi-nucleate or quadrinucleate and their nuclear structure is like that of trophozoites. The nucleus of a matured cyst, on the other hand, is very small and it is difficult to differentiate its detailed structure. It shows a very small karyosome and a delicate nuclear membrane.
The characteristic of the cysts of Entamoeba histolytica is the presence of chromatoid bodies, which occur either singly or in multiples of two or more. These chromatoid bodies occur in the early stages of the cysts and disappear in the mature quadrinucleate type.
3. Reproduction of Entamoeba:
Reproduction in Entamoeba occurs by simple binary fission, where the nucleus divides first followed by the body of the organism (Fig 1.13). The larger trophic form, infecting the intestinal mucosa, reproduces by binary fission. Multiplication also takes place by cyst formation that takes place in the lumen of the intestine, before coming out with the faeces.

4. Life Cycle of Entamoeba:
E. histolytica is a monogenetic parasite as it completes its whole life cycle within a single host, i.e. man. Its life cycle consists of three stages trophozoite or vegetative, pre-cystic and cystic stages. The mature quadrinucleate cysts are the infective forms of the parasite.
When a person swallows contaminated food and drink, the fully developed cysts pass unaltered through the stomach, as the cyst wall is resistant to the action of the gastric juice. The cyst wall is finally digested by the action of trypsin in the intestine. When the cyst reaches the caecum excystation takes place.
During excystation, the cytoplasmic body retracts from the cyst wall and becomes loose. Vigorous amoeboid movement results and a cut appears in the cyst wall through which a mass of cytoplasm protrudes and ultimately the whole body comes out.
The four nucleated amoeba that emerges from the cyst (Fig. 1.13) eventually forms eight amoebulae (metacystic trophozoites) by the division of the nuclei with successive fission of the cytoplasm.
The young, motile trophozoites, work their way down through the iliocaecal valve, to the mucous membrane of the gut and develop into large active trophozoite. They then invade the tissues and enter through the crypts of Lieberkuhn, penetrate the muscularis mucosae and lodge themselves in the sub-mucous tissue. They are exclusively parasitic, growing at the expense of living tissues and multiplying by binary fission.
It is not the aim of the protozoan parasite to cause death of the host in which it has parasitized. But, sometimes trophozoites may invade the liver where they may colonies and may be responsible for the death of the host.
However, the primary aim of the parasitic cycle is to propagate its own species and therefore, a certain number of trophozoites is discharged into the lumen of the bowel and is transformed into small pre-cystic forms from which the cysts are developed.
The whole process of encystation takes place in a few hours and the mature cyst in the bowel can survive for about 2 days. The cysts are unable to develop further in the same host, but when introduced into another individual they repeat the above stated cycle.
5. Pathogenicity of Entamoeba:
Nearly all parasites cause some disease or the other to its host. These effects or symptoms are called pathological effects, such parasites are known as pathogenic and the phenomenon is known as pathogenicity.
Mode of Infection:
Transmission of E. histolytica from an infected man to a healthy man is effected through its encysted stage and infection occurs through the ingestion of these cysts. Faecal contamination of drinking water, vegetables and food is the prime route of infection.
Source of Infection:
Directly or indirectly flies convey the infection. These insects while passing from faeces to unprotected food-stuffs carry the cysts mechanically. Droppings of cockroaches have also been found to contain the cysts of this parasite and therefore, also serve as a source of infection.
Reservoirs of Infection:
Natural infection of this protozoan parasite is seen only in man and monkey. Man is the commonest source of infection. Dogs, monkeys and lower animals like rats have also been regarded as reservoirs of E. histolytica.
Incubation Period:
In man, the incubation period is generally four or five days. In cats the incubation period is two days to about two weeks.
Pathogenic Lesions:
i. Amoebic Dysentery:
It is the primary or intestinal amoebiasis resulting in diarrhoea. The infection is limited entirely to the large intestine. The parasite attacks the intestinal mucosa that results into ulceration and dysentery. The parasite secretes a tissue-dissolving enzyme, which destroys the intestinal epithelial lining causing necrosis.
The stool of a person suffering from amoebic dysentery is generally acidic and contains mainly blood mucus and a large number of trophozoites.
ii. Secondary Amoebic Infection:
Secondary infections take place when Entamoeba in their progress through the tissues of the intestine enter into the portal vein and are carried to the liver, (Hepatic amoebiasis) which acts as first filter. If the liver fails to act as an efficient filter, Entamoeba may travel beyond the liver and enter into the hepatic veins from the portal capillaries and ultimately enters into the pulmonary circulation.
They may then be arrested in the lungs (Pulmonary amoebiasis) which acts as second filter. Some, however, may escape from the pulmonary capillaries, enter the systemic circulation and may localize in the brain (Cerebral amoebiasis). Other places where Entamoeba have also been detected are urinary tract, spleen and epidydirnis.
Therapeutic Treatment:
The main aim is to eradicate the causative organism (E. histolytica) by means of specific therapy with certain drugs.
These drugs may be divided into three main groups:
a. Alkaloids of Ipecacuanha and Kurchi
b. Pentavalent arsenicals—Stovarsol and carbarsone
c. Quinoline derivatives—Chiniofon (yatren), vioform and diodoquin.